
Who is this information for?
This information is for patients, families and carers of patients with inner disorders who may benefit from the use of Corticosteroid Therapy (CT) for Inner Ear Disorders, including:
- Sudden Sensorineural Hearing Loss (SSNHL)
- (see additional MEG info sheet)
- Endolymphatic Hydrops, including Cochlear Hydrops and Autoimmune Inner Ear Disorders
- (see additional MEG Info sheet)
- Meniere’s Disease
- (see additional MEG Info sheet)
Background:
- What are corticosteroids?
- Corticosteroids are man-made drugs that work like cortisol, a natural steroid hormone in your body.
- These medicines reduce inflammation and alter the immune system.
- They can be taken as tablets, or injected into the blood-stream or body tissues.
- Common examples of corticosteroids include: Prednisolone (e.g. Solone®, Panafcortelone®) Dexamethasone & Triamcinolone (e.g. Kenalog®, Kenacort®)
- Corticosteroid Therapy (CT) is a well known therapeutic option for patients with acute inner
ear disorders affecting cochlear and/or vestibular function; causing hearing loss, tinnitus,
vertigo and / or unbalance and aural fullness. - Sensorineural hearing loss (new onset or sudden deterioration of pre-existing SNHL) should be confirmed with an Audiogram prior to commencing CT.
- After Sudden Sensorineural Hearing Loss (SSNHL), spontaneous improvement (without any intervention) can occur in up to 30% of cases.
- Medical treatment with Corticosteroid therapy can double the possibility of recovery (up to 60%)
- Patients with poorer prognosis are those who suffer severe or profound sensorineural hearing loss and those who are over 60 years of age.
Therapeutic recommendations
- Corticosteroid Therapy is most beneficial the sooner it is started after symptoms onset.
- For Sudden Sensorineural Hearing Loss, corticosteroid use should start ideally within 72 hours of deafness onset (1), and can be offered within 2 weeks of symptom onset as a primary treatment.
- Salvage treatment, which is given to patients who did not receive or did not respond to primary treatment, is typically delivered 2-6 weeks after the onset of symptoms. Often it is given in three doses that are 1-2 weeks apart.
- Initial administration route is systemic (oral) with topic therapy (Trans-Tympanic) used as salvage.
- Systemic Use
- Prednisone (1 mg / kg / day ) or Dexamethasone (10mg / day) should be used for at least 7-14 days, with a tapering of the dose over a similar time period, provided there are no contraindications for its use (2).
- The medication should be used in the morning, after breakfast.
- Topical Use
- Administration of Trans-Tympanic Steroid Therapy is recommended in the following cases:
- Failure with Systemic CT
- Presence of contraindications for Systemic use of CT
- Previous good response to Trans-Tympanic and repeat need for its use.
- Hearing loss duration for more than 2 weeks
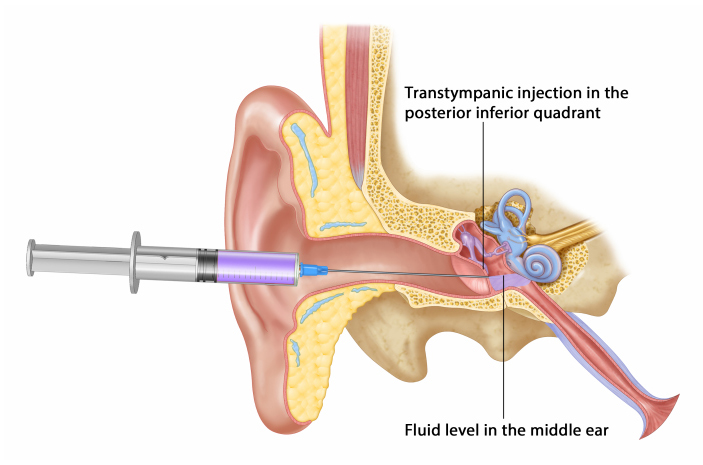
- Application modality
- First, your Specialist surgeon at MEG will apply a local anaesthetic into your ear canal – either a cream, a spray, or an injection
- e.g. EMLA: Lignocaine/Prilocaine cream mix or
- e.g. 10% Lignocaine Spray - Dexamethasone (24 mg / mL solution) will be injected through the tympanic membrane (or a patent grommet) into the middle ear, applying about 0.5 cc per injection procedure.
- First, your Specialist surgeon at MEG will apply a local anaesthetic into your ear canal – either a cream, a spray, or an injection
- Administration of Trans-Tympanic Steroid Therapy is recommended in the following cases:
AFTER CARE
Immediately after the injection
- Rest lying on your side for at least 30 minutes is recommended to assist maximal possible absorption into the inner ear.
- Many patients will feel dizzy straight after injection, this will normally settle in minutes to hours.
Within the first 24 hours
- It is normal to hear liquid moving in the ear or feel is tripping into the nose. This may make sounds more muffled for the first couple of days.
- Avoid blowing your nose for the rest of the day
- Avoid driving, use of heavy machinery or heavy object lifting
- Use paracetamol/ibuprofen for pain relief, if required at home
Within the first 72 hours
- Keep the injected ear dry by using a water proof ear plug, for at least 3 days, following the injection, or for the time period advised by your Specialist Surgeon.
What should I expect?
- Minor discharge and bleeding from the treated ear may be noticed for short period of time.
- Any improvement in symptoms is not immediate and may take hours, days or sometimes even weeks to be noticed.
Repeat topical administration
- Further weekly injections (usually two) can be arranged with your Specialist Surgeon if ear symptom improvement is noticed (confirmed on repeat Audiometry hearing test) after 7 days of the first injection.
- Discussion of further benefit vs. risks of the procedure will be again discussed with your specialist before having additional applications.
Potential risks of Corticosteroid Therapy (See separate MEG info sheet for more detail)
- Systemic use
- Insomnia
- Aggravation of pre-existing mood disorders
- Glaucoma
- Gastric reflux
- Gastric ulcer
- Gastrointestinal bleed
- Elevation of Blood sugar and lipid levels
- Avascular femoral head necrosis
- Transtympanic injection
- Ear pain
- Residual Eardrum Perforation (hole in the eardrum)
- Cholesteatoma Formation (‘skin’ of the eardrum growing inwards into the middle ear)
- Tympanosclerosis (ear drum scar)
Therapy failure and need for further treatment
Please note there we cannot guarantee either the effectiveness or duration of Corticosteroid therapy in any case.
Your Specialist surgeon will discuss with your further rehabilitation options in case of failure of medical therapy, which may include, hearing rehabilitation options, including conventional hearing amplification (ie Hearing aids), Hearing implants and Vestibular physiotherapy.
Concerns or questions?
You can contact your ENT Specialist at the Melbourne ENT Group (MEG):
- Phone: 1300- 952-808
- Email: admin@melbentgroup.com.au
- Website: www.melbentgroup.com.au
Your GP is also the best contact for ongoing care and concerns.
Further information
The Department of Health has published a guide on different causes of hearing loss.
This is available online at https://www.betterhealth.vic.gov.au/health/ConditionsAndTreatments/deafness-a-range-ofcauses